Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study
This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain and weight loss, anorexia, and subjective fevers. During the clinical examination, the patient was found to have ascites, bilateral pleural effusion, fever, and a general deterioration in her condition. Blood tests revealed normochromic normocytic anemia. The C-reactive protein was elevated, and the erythrocyte sedimentation rate was accelerated. Ferritin levels were raised. Her blood sugar, hepatic and renal functions were normals. The electrolyte panel showed no abnormalities. Serologies for hepatitis B, C, and HIV were negative, and the immunological profile was normal. The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative. Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated. Additionally, the CA125 level was significantly elevated, exceeding 600 UI/ml. A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm. The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion. The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. Anatomopathology confirmed peritoneal tuberculosis. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
. Peritoneal tuberculosis is uncommon, making it the fourth most frequent type of extrapulmonary tuberculosis. Diagnosing this form of the disease can be particularly difficult due to the non-specific nature of its clinical and radiological signs
[2]
Zaman K. Tuberculosis: a global health problem. J Health PopulNutr. 2010; 28(2): 111–113.
. In its pseudotumoral pelvic form, it shows many clinical, biological, and radiological similarities with ovarian cancer, which is the main differential diagnosis
[3]
Lantheaume S, Soler S, Issartel B, et al. Disseminated peritoneal tuberculosis simulating ovarian cancer: about a case. Obs, Gyn and Fertility. 2003; 31(7-8): 624–626.
In this study, we report the case of a patient with peritoneal tuberculosis that mimicked advanced ovarian neoplasia to highlight the diagnostic challenges and underscore the value of laparoscopy in such cases.
2. Case Study
This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain in the context of weight loss, anorexia, and subjective fevers.
During the clinical examination, the patient was found to have ascites without any signs of portal hypertension, heart failure, or nephropathy. She also had bilateral pleural effusion, fever, and a general deterioration in her condition, classified as stage 2 by the World Health Organization (WHO) guidelines. Her lymph nodes were not enlarged, and no skin abnormalities were observed. Additionally, her joints were flexible, and her neurological examination showed normal results.
Blood tests revealed normochromic normocytic anemia with a hemoglobin level of 10.3 g/dl. The C-reactive protein (CRP) was elevated at 128 mg/l, and the erythrocyte sedimentation rate was accelerated at 93 mm/hr. Ferritin levels were significantly raised at 1363.7 ng/ml. AST levels were measured at 41 UI/l and ALT at 21 UI/L. Her blood sugar and renal function were normal, with a creatinine level of 10 mg/l. The electrolyte panel showed no abnormalities, with sodium at 140 meq/L and potassium at 3 meq/L. Serologies for hepatitis B, C, and HIV (Human immunodefficiency virus) were negative, and the immunological profile was normal.
The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative.
Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated at 79.34 UI/l. Additionally, the CA125 (cancer antigen125) level was significantly elevated, exceeding 600 UI/ml.
A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm.
The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion, thickening of the peritoneal layers compatible with peritoneal carcinosis lesions, and a bilateral pleural effusion of low abundance with no signs of secondary spread to the liver, lungs, or bones.
The diagnosis strongly suggested advanced ovarian neoplasia with peritoneal carcinomatosis, but tuberculosis was also considered a possibility.
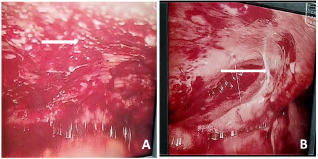
The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. (See figure)
Figure 1. Laparoscopic view displaying multiple whitish peritoneal nodules on the peritoneum (A) and adhesions (B).
Biopsy samples were taken, and the histopathological examination revealed a tuberculous granuloma in the peritoneal wall. It consisted of foci of eosinophilic necrosis surrounded by epithelioid histiocytes and Langhans giant cells.
Antituberculosis treatment was initiated following a protocol that combined Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), and Ethambutol (E) for two months, followed by a combination of RH for four months.
Under antituberculosis treatment, the patient showed significant clinical improvement, including the cessation of fever, restored appetite, weight gain, and a notable decrease in both ascites and pleural effusion.
Paraclinical findings showed a return to normal in the biological parameters, including the CA125 levels.
3. Discussion
Tuberculosis remains a significant public health issue in Senegal, despite considerable efforts by public authorities to combat this disease, particularly in its pulmonary form, which is responsible for its contagiousness. Extrapulmonary forms of tuberculosis often pose diagnostic challenges due to their variable clinical presentations. The peritoneal pseudotumoral localization of tuberculosis is a rare clinical form, with an estimated frequency of 1 to 3% according to series
[2]
Zaman K. Tuberculosis: a global health problem. J Health PopulNutr. 2010; 28(2): 111–113.
Several factors may contribute to its development, such as HIV infection, prolonged corticosteroid therapy, low socio-economic status, treatment with immunosuppressants, and BCG therapy
[6]
Eghdami L, Kwon J. Tuberculose péritonéale se présentant sous forme d´une ascite persistante. J Obstet Gynaecol Can. 2015; 37(4): 296.
Pommier J-D, Joly V. Complications following intravesical Bacillus Calmette-Guérin therapy: Epidemiology, clinical features and medical care. Anti-infectives journal. 2016; 18: 106–116.
. With our patient, no risk factor was identified.
The clinical signs are non-specific, including abdominal pain, intestinal transit disorders, and menstrual disturbances that may manifest as dysmenorrhea or amenorrhea. Fever, either isolated or associated with chills or profuse night sweats, may be observed. A deterioration in general health can manifest as asthenia, anorexia, or significant weight loss, sometimes very severe. Clinical examination often reveals the presence of isolated, free ascites. An association with other locations, particularly pulmonary or digestive, should be investigated, although it is absent in 30 to 50% of cases
[8]
Saadi H, Mamouni M, Errarhay S, et al. Pseudotumoral pelvoperitoneal tuberculosis: about four cases. PAMJ. 2012; 13: 52. PMID: 23330043.
[8]
. The clinical presentation of our patient included chronic abdominal pain and isolated ascites with fever and weight loss.
Like the clinical signs, the biological findings are non-specific. An inflammatory syndrome of varying intensity is often noted, as observed in this case.
CA125, a high molecular weight glycoprotein, is expressed by a large proportion of epithelial ovarian cancers
[10]
Daaloul W, Gharbi H, Ouerdiane N, et al. Tuberculose péritonéale disséminée simulant un cancer ovarien. La tunisie méd. 2012; 90(04): 333–335. PMID: 22535355.
[10]
. Its elevation in peritoneal tuberculosis can mistakenly suggest a diagnosis of ovarian cancer, potentially delaying the correct diagnosis, as was the case with our patient.
The ascitic fluid is usually yellowish in color, exudative, and predominantly lymphocytic
[11]
Amouri A, Boudabbous M, Mnif L, Tahri N. Current profile of peritoneal tuberculosis: study of a Tunisian series of 42 cases and review of the literature.. J int med. 2009; 30: 215-220.
The elevation of ADA (adenosine deaminase) in peritoneal fluid has a sensitivity and specificity of 100% and 97%, respectively, for the diagnosis of peritoneal tuberculosis in the absence of cirrhosis (86). Its positivity in this patient was a presumptive factor.
The Polymerase Chain Reaction (PCR) test and gene amplification reaction using cerebrospinal fluid (CSF) can isolate the Mycobacterium tuberculosis (BK) in 24 to 48 hours, but these tests are expensive and have reduced sensitivity
[4]
Abdallah M, Larbi T, Hamzaoui S, et al. Tuberculose abdominale: étude retrospective de 90 cas. La revue de medecine interne. 2011 Apr; 32(4): 212–217.
. This could explain its negativity in this context.
Imaging techniques like ultrasound and computed tomography (CT) can sometimes aid in diagnosis. Specifically, findings such as ascites with septations, peritoneal thickening with heterogeneous enhancement, the presence of hypodense areas indicating caseous necrosis, and lymphadenopathy can suggest a tuberculous origin. Additionally, the presence of pleuroparenchymal sequelae of pulmonary tuberculosis (as observed in our patient), and less frequently, active lesions, also support this diagnosis
[9]
Vardareli E, Kebapci M, Saricam T, et al. Tuberculous peritonitis of the wet ascitic type: clinical features and diagnostic value of image-guided peritoneal biopsy. Dig Liver Dis. 2004; 36(3): 199–204.
. The exploration of the peritoneal cavity typically reveals whitish granulations, peritoneal nodules, hyperemia of the peritoneum, filamentous peritoneal adhesions, and agglutination of intestinal loops. A laparoscopy performed on our patient visualized peritoneal nodules.
The histological study of the biopsy samples reveals epithelioid giant cell granulomas, typically with caseous necrosis
[7]
Pommier J-D, Joly V. Complications following intravesical Bacillus Calmette-Guérin therapy: Epidemiology, clinical features and medical care. Anti-infectives journal. 2016; 18: 106–116.
. This confirms the diagnosis in accordance with the findings of this observation.
The treatment of peritoneal tuberculosis is based on a four-drug anti-tuberculosis regimen: RHZE for 2 months, followed by a two-drug regimen of RH for 4 months. Under this protocol, our patient showed good clinical and biological improvement
[9]
Vardareli E, Kebapci M, Saricam T, et al. Tuberculous peritonitis of the wet ascitic type: clinical features and diagnostic value of image-guided peritoneal biopsy. Dig Liver Dis. 2004; 36(3): 199–204.
Amouri A, Boudabbous M, Mnif L, Tahri N. Current profile of peritoneal tuberculosis: study of a Tunisian series of 42 cases and review of the literature.. J int med. 2009; 30: 215-220.
Marshall JB. Tuberculosis of the gastrointestinal tract and peritoneum. Am J Gastroenterol. 1993; 88(7): 989–999. PMID: 8317433.
[9, 11, 12]
.
4. Conclusion
Tuberculosis remains a public health issue in Senegal. Extrapulmonary locations often present a diagnostic challenge due to the non-specific nature of their clinical presentation. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
Abbreviations
WHO
World Health Organization
CRP
C Reactive Protein
HIV
Human Immunodeficiency Virus
ADA
Adenosine Deaminase
CT
Computed Tomography
DNA
Desoxyribonucleic Acid
ALT
Aminotransferase Alanine
AST
Aminotransferase Aspartate
CA125
Cancer Antigen 125
R
Rifampicin
H
Isoniazid
Z
Pyrazinamide
E
Ethambutol
Author Contributions
Jean Noel Diokel Ndour: Conceptualization, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing
Pommier J-D, Joly V. Complications following intravesical Bacillus Calmette-Guérin therapy: Epidemiology, clinical features and medical care. Anti-infectives journal. 2016; 18: 106–116.
Saadi H, Mamouni M, Errarhay S, et al. Pseudotumoral pelvoperitoneal tuberculosis: about four cases. PAMJ. 2012; 13: 52. PMID: 23330043.
[9]
Vardareli E, Kebapci M, Saricam T, et al. Tuberculous peritonitis of the wet ascitic type: clinical features and diagnostic value of image-guided peritoneal biopsy. Dig Liver Dis. 2004; 36(3): 199–204.
Daaloul W, Gharbi H, Ouerdiane N, et al. Tuberculose péritonéale disséminée simulant un cancer ovarien. La tunisie méd. 2012; 90(04): 333–335. PMID: 22535355.
[11]
Amouri A, Boudabbous M, Mnif L, Tahri N. Current profile of peritoneal tuberculosis: study of a Tunisian series of 42 cases and review of the literature.. J int med. 2009; 30: 215-220.
Ndour, J. N. D., Diallo, B. M., Ndiaye, Y., Faye, F. A., Nana, M. B., et al. (2024). Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. American Journal of Internal Medicine, 12(5), 78-81. https://doi.org/10.11648/j.ajim.20241205.13
Ndour, J. N. D.; Diallo, B. M.; Ndiaye, Y.; Faye, F. A.; Nana, M. B., et al. Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. Am. J. Intern. Med.2024, 12(5), 78-81. doi: 10.11648/j.ajim.20241205.13
Ndour JND, Diallo BM, Ndiaye Y, Faye FA, Nana MB, et al. Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. Am J Intern Med. 2024;12(5):78-81. doi: 10.11648/j.ajim.20241205.13
@article{10.11648/j.ajim.20241205.13,
author = {Jean Noel Diokel Ndour and Bachir Mansour Diallo and Yanidou Ndiaye and Fulgence Abdou Faye and Mamoudou Baba Nana and Atoumane Faye and Adama Berthé and Papa Souleymane Touré and Madoky Magatte Diop and Mamadou Mourtalla Ka},
title = {Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study
},
journal = {American Journal of Internal Medicine},
volume = {12},
number = {5},
pages = {78-81},
doi = {10.11648/j.ajim.20241205.13},
url = {https://doi.org/10.11648/j.ajim.20241205.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20241205.13},
abstract = {This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain and weight loss, anorexia, and subjective fevers. During the clinical examination, the patient was found to have ascites, bilateral pleural effusion, fever, and a general deterioration in her condition. Blood tests revealed normochromic normocytic anemia. The C-reactive protein was elevated, and the erythrocyte sedimentation rate was accelerated. Ferritin levels were raised. Her blood sugar, hepatic and renal functions were normals. The electrolyte panel showed no abnormalities. Serologies for hepatitis B, C, and HIV were negative, and the immunological profile was normal. The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative. Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated. Additionally, the CA125 level was significantly elevated, exceeding 600 UI/ml. A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm. The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion. The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. Anatomopathology confirmed peritoneal tuberculosis. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
},
year = {2024}
}
TY - JOUR
T1 - Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study
AU - Jean Noel Diokel Ndour
AU - Bachir Mansour Diallo
AU - Yanidou Ndiaye
AU - Fulgence Abdou Faye
AU - Mamoudou Baba Nana
AU - Atoumane Faye
AU - Adama Berthé
AU - Papa Souleymane Touré
AU - Madoky Magatte Diop
AU - Mamadou Mourtalla Ka
Y1 - 2024/10/18
PY - 2024
N1 - https://doi.org/10.11648/j.ajim.20241205.13
DO - 10.11648/j.ajim.20241205.13
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 78
EP - 81
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20241205.13
AB - This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain and weight loss, anorexia, and subjective fevers. During the clinical examination, the patient was found to have ascites, bilateral pleural effusion, fever, and a general deterioration in her condition. Blood tests revealed normochromic normocytic anemia. The C-reactive protein was elevated, and the erythrocyte sedimentation rate was accelerated. Ferritin levels were raised. Her blood sugar, hepatic and renal functions were normals. The electrolyte panel showed no abnormalities. Serologies for hepatitis B, C, and HIV were negative, and the immunological profile was normal. The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative. Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated. Additionally, the CA125 level was significantly elevated, exceeding 600 UI/ml. A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm. The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion. The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. Anatomopathology confirmed peritoneal tuberculosis. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
VL - 12
IS - 5
ER -
Ndour, J. N. D., Diallo, B. M., Ndiaye, Y., Faye, F. A., Nana, M. B., et al. (2024). Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. American Journal of Internal Medicine, 12(5), 78-81. https://doi.org/10.11648/j.ajim.20241205.13
Ndour, J. N. D.; Diallo, B. M.; Ndiaye, Y.; Faye, F. A.; Nana, M. B., et al. Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. Am. J. Intern. Med.2024, 12(5), 78-81. doi: 10.11648/j.ajim.20241205.13
Ndour JND, Diallo BM, Ndiaye Y, Faye FA, Nana MB, et al. Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study. Am J Intern Med. 2024;12(5):78-81. doi: 10.11648/j.ajim.20241205.13
@article{10.11648/j.ajim.20241205.13,
author = {Jean Noel Diokel Ndour and Bachir Mansour Diallo and Yanidou Ndiaye and Fulgence Abdou Faye and Mamoudou Baba Nana and Atoumane Faye and Adama Berthé and Papa Souleymane Touré and Madoky Magatte Diop and Mamadou Mourtalla Ka},
title = {Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study
},
journal = {American Journal of Internal Medicine},
volume = {12},
number = {5},
pages = {78-81},
doi = {10.11648/j.ajim.20241205.13},
url = {https://doi.org/10.11648/j.ajim.20241205.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20241205.13},
abstract = {This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain and weight loss, anorexia, and subjective fevers. During the clinical examination, the patient was found to have ascites, bilateral pleural effusion, fever, and a general deterioration in her condition. Blood tests revealed normochromic normocytic anemia. The C-reactive protein was elevated, and the erythrocyte sedimentation rate was accelerated. Ferritin levels were raised. Her blood sugar, hepatic and renal functions were normals. The electrolyte panel showed no abnormalities. Serologies for hepatitis B, C, and HIV were negative, and the immunological profile was normal. The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative. Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated. Additionally, the CA125 level was significantly elevated, exceeding 600 UI/ml. A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm. The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion. The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. Anatomopathology confirmed peritoneal tuberculosis. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
},
year = {2024}
}
TY - JOUR
T1 - Exploring the Diagnostic Challenges of Pseudotumoral Peritoneal Tuberculosis That Mimics Advanced Ovarian Cancer in Women: The Role of Laparoscopy in a Case Study
AU - Jean Noel Diokel Ndour
AU - Bachir Mansour Diallo
AU - Yanidou Ndiaye
AU - Fulgence Abdou Faye
AU - Mamoudou Baba Nana
AU - Atoumane Faye
AU - Adama Berthé
AU - Papa Souleymane Touré
AU - Madoky Magatte Diop
AU - Mamadou Mourtalla Ka
Y1 - 2024/10/18
PY - 2024
N1 - https://doi.org/10.11648/j.ajim.20241205.13
DO - 10.11648/j.ajim.20241205.13
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 78
EP - 81
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20241205.13
AB - This case involves a 63-year-old multiparous woman with no significant medical history and no known exposure to tuberculosis. She presented with chronic abdominal pain and weight loss, anorexia, and subjective fevers. During the clinical examination, the patient was found to have ascites, bilateral pleural effusion, fever, and a general deterioration in her condition. Blood tests revealed normochromic normocytic anemia. The C-reactive protein was elevated, and the erythrocyte sedimentation rate was accelerated. Ferritin levels were raised. Her blood sugar, hepatic and renal functions were normals. The electrolyte panel showed no abnormalities. Serologies for hepatitis B, C, and HIV were negative, and the immunological profile was normal. The ascitic tap yielded a citrine-yellow fluid, and the cytochemical analysis indicated that the ascites were exudative. Analysis of the ascitic fluid revealed that the DNA test for Mycobacterium tuberculosis was negative, but the adenosine deaminase (ADA) level was elevated. Additionally, the CA125 level was significantly elevated, exceeding 600 UI/ml. A pelvic ultrasound identified a cystic pelvic mass with thick septations but without any solid tissue component, measuring 92x69 mm. The complementary CT (Computed Tomography) scan revealed enlarged ovaries, heterogeneous on the left, associated with a moderately abundant peritoneal effusion. The laparoscopic exploration revealed inflammatory peritoneal nodules, parietal adhesions, and serous ascites. Anatomopathology confirmed peritoneal tuberculosis. The peritoneal form, particularly in its pseudotumoral manifestation, can mimic ovarian cancer. Definitive diagnosis often requires invasive procedures.
VL - 12
IS - 5
ER -